Search for articles:
Junlei Li
Corresponding authors:
Received: 2018-10-24
Revised: 2019-02-28
Accepted: 2019-04-28
Online: 2020-01-01
Copyright: 2020 Editorial board of Journal of Materials Science & Technology Copyright reserved, Editorial board of Journal of Materials Science & Technology
More
Abstract
Bone plates play a vital role in bone fracture healing by providing the necessary mechanical fixation for fracture fragments through modulating biomechanical microenvironment adjacent to the fracture site. Good treatment effect has been achieved for fixation of bone fracture with conventional bone plates, which are made of stainless steel or titanium alloy. However, several limitations still exist with traditional bone plates including loosening and stress shielding due to significant difference in modulus between metal material and bone tissue that impairs optimal fracture healing. Additionally, due to demographic changes and non-physiological loading, the population suffering from refractory fractures, such as osteoporosis fractures and comminuted fractures, is increasing, which imposes a big challenge to traditional bone plates developed for normal bone fracture repair. Therefore, optimal fracture treatment with adequate fixation implants in terms of materials and design relevant to special conditions is desirable. In this review, the complex physiological process of bone healing is introduced, followed by reviewing the development of implant design and biomaterials for bone plates. Finally, we discuss recent development of hybrid bone plates that contains bioactive elements or factors for fracture healing enhancement as a promising direction. This includes biodegradable Mg-based alloy used for designing bone screw-plates that has been proven to be beneficial for fracture healing, an innovative development that attracts more and more attention. This paper also indicates that the tantalum bone plates with porous structure are also emerging as a new fracture internal fixation implants. The reduction of the stress shielding is verified to be useful to accelerate bone fracture healing. Potential application of biodegradable metals may also avoid a second operation for implant removal. Further developments in biometals and their design for orthopedic bone plates are expected to improve the treatment of bone fracture, especially the refractory fractures.
Keywords:
Bone fractures are most commonly seen on patients with traumatic injuries [1]. Bone fracture healing is a complex physiologic process involving a cascade events, including interplay of various cellular and biomechanical factors [2]. Approximately 5%-10% of bone fractures will not heal normally, and delayed healing or fracture non-union are therefore quite common [3].
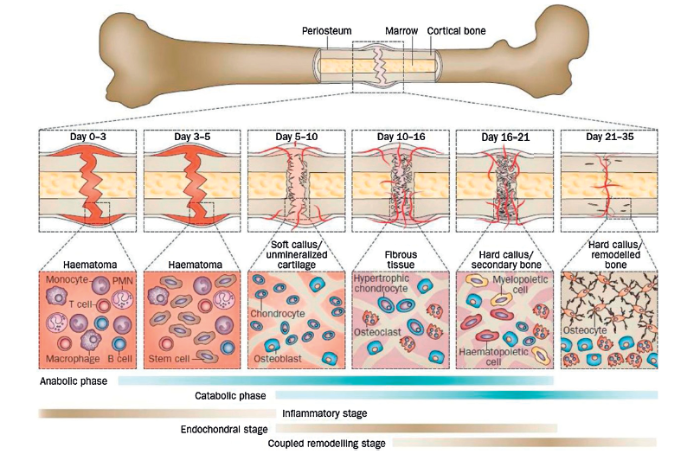
There are two patterns of bone fracture healing, i.e., primary healing and secondary healing [4]. Primary healing means a direct attempt by the cortex to re-establish itself once it has been interrupted although it is rarely occur [5]. Primary healing occurs only when there is anatomic restoration of the fracture fragments by rigid internal fixation, and interfragmentary strain should be sustained at the micrometric level [2]. The majority of fractures will be healed by secondary healing, which involves responses in the periosteum and external soft tissues with the subsequent formation of a callus. This type of healing benefits from micromotion, but it can be suppressed by stiff fixation [3]. Secondary healing involves a combination of intramembranous and endochondral ossification where these two processes participate in the fracture repair sequence by at least five discrete healing stages, as summarized in Fig. 1 [6].
Fig. 1. Biological events of closed femur fracture healing for a mouse, and the cell types are involved at each stage of fracture healing. Abbreviations: PMN, polymorphonuclear leucocyte. Reprinted from Ref. [
In the first few hours after fracture, acute inflammation occurs in the soft tissue surrounding the fracture [7]. Subsequently, hematoma forms within the fracture gap [8]. Multiple types of cells related to inflammation and immunity emerge inside the hematoma. These cells release various biological factors to initiate the cascades of cellular events [9]. Subsequently, osteoprogenitor cells and bone mesenchymal stem cells (MSCs) adjacent to the fracture line differentiate primarily into chondrocytes and few osteoblasts. The hematoma tissue will be replaced by the cartilage callus [1]. At the same time, a hard callus forms in the subperiosteal area through intramembranous ossification. Then, chondrocytes become hypertrophic, release calcium and undergo apoptosis, and endochondral ossification occurs [2,10]. Monocytes differentiate into osteoclast-like cells, which resorb the calcified cartilage, and MSCs differentiate into osteoblasts, which fill the resorption lacunae with new bone. These processes lead to the formation of woven bone with a trabecular structure. In this process, the cartilaginous callus is taken over by a hard callus [4]. Following these processes, the bone remodeling begins with coordinated osteoblast and osteoclast activities over a period of several months where the fracture callus are remodeled towards lamellar bone [6].
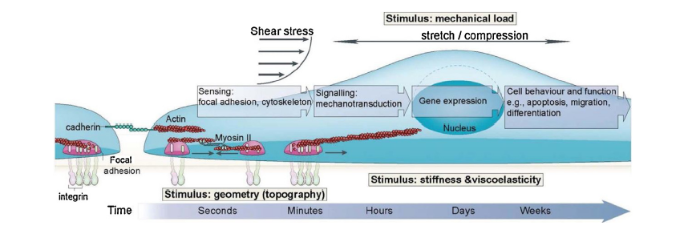
As shown in Fig. 2, mechanical stimuli, such as stress, strain, topography, stiffness and viscoelasticity, play an important role in the physiological process of bone fracture healing [12]. The mechanism of the transduction from the mechanical microenvironment to cellular behavior is a popular and cutting-edge research topic at present [11,[13], [14], [15]]. The fixation methods, which are closely associated with the mechanical microenvironment at the fracture site, have regulatory effects on the cellular bioactivity of the osteoblasts, chondrocytes, endothelial cells, fibroblasts and MSCs. Furthermore, the fixation methods play a guiding role in fracture healing behavior [16,17]. It was reported that the overall stability of the fixation and immobilization of the fracture affected the patterns of MSC differentiation into chondrocytes or osteoblasts, with more-extensive cartilage tissue formation associated with less fracture stability while more bone tissue associated with increasing fracture stability [6,18].
Fig. 2. Mechanotransduction converts mechanical stimuli into chemical signals to regulate cell behavior and function. Reprinted from Ref. [
Fracture healing at different locations has different local environments. It is desirable to select suitable fixation methods and create an optimal environment to meet the targeted healing requirements [17]. Fracture healing along the diaphysis, which is oriented for fast recovery of load bearing function, is generally achieved by way of secondary bone healing. During this process, there is callus formation, but it is unlikely to interfere with the mechanical function [16]. For intra-articular fracture, a callus should be avoided in order to prevent its adverse effects on joint function. Therefore, primary bone healing, which does not induce a callus, is preferred [16]. There are two forms of fracture fixation: external fixation and internal fixation. In the procedure of external fixation, there is no need to open the tissue. Interfragmentary immobilization can be achieved by splints, plaster casts, external fixation braces and so on. For internal fixation, the tissue adjacent to the fracture has to be opened, and an anatomical reduction of the fragment should be carried out prior to implantation of internal fixation devices, such as wires, pins, screws, and bone plates [19].
Fixation using different devices may have different levels of stability [20]. Absolute stability is required for achieving primary healing experimentally, and less stability is necessary for realization of secondary healing. However, excessive interfragmentary instability will impede cartilage replacement, diminish angiogenesis and prevent bone from bridging the fracture gap. Therefore, an optimal ‘window’ of interfragmentary motion seems to be needed to enable normal calluses to develop and stably bridge a fracture [6].
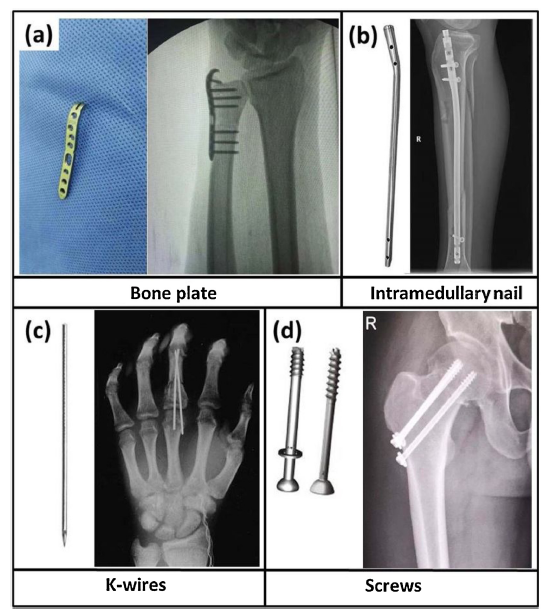
The global market of fracture fixation devices is estimated at $5.5 billion, according to published statistics [21]. The medical devices used for fracture fixation include plates, intramedullary nails, pins, wires, screws, etc., as shown in Fig.3. Different fracture sites are commonly recommended to be treated using different internal fixation methods (Table 1) [22].
Fig. 3. Common medical devices used for fracture internal fixation. (a) Bone plate used for the fixation of ulnar fracture ; (b) Intramedullary nail used for the fixation of tibial fracture; (c) K-wire used for the fixation of phalangeal fracture; (d) Screws used for the fixation of femoral neck fracture.
Table 1 Different fracture sites using different internal fixation methods [
| Fracture sites | Internal fixators | |
|---|---|---|
| Head | Skull fracture Craniofacial fracture | Wires, pins and plates Wires, screws and plates |
| Trunk | Clavicle fracture Scapular fracture Pelvic fracture Spinal fracture | Intramedullary nail and plates Screws and plates Screws, plates and external fixators Fixation device consists of rods, pedicle screws and plates |
| Upper limb fracture | Humeral fracture Radius, ulnar fracture Metacarpal and phalangeal fracture | Open reduction with plate and screws/close reduction with intramedullary nail Open reduction with plate and screws/close reduction with intramedullary nail Close reduction with external fixators, open reduction with intramedullary nail, screws and plates |
| Lower limb fracture | Femoral fracture Tibial and fibular fracture Metatarsus fracture Calcaneal fracture | Open reduction with plate and screws/close reduction with intramedullary nail Open reduction with plate and screws and intramedullary nail Open reduction with plate and screws and intramedullary nail Close reduction and fixation with screws or wires |
1.3.1. Bone plates
Bone plates are the most common implants in internal fixation [23], showing many advantages, such as sufficient stability, tension resistance, compression resistance, shear resistance, torsion resistance and bending resistance, for plates and screws used as internal fracture fixation implants [24]. Common surgical procedures for the plate include open reduction and internal fixation and bridge fixation. Open reduction and internal fixation is anatomical reduction, but it leads to extensive destruction of soft tissue and blood supply. And even sometimes, it is necessary to extend the preoperative time to optimize soft tissue recovery. Bridge fixation technology brings less soft tissue injury than open reduction, but it also has a higher rate of fracture malformation and increased local soft tissue pressure possibility [[25], [26], [27], [28]]. To satisfy the bone healing requirements under proper biomechanical microenvironment, the structure and materials of bone plates have gone through a long evolution. Conventional plates, which rely on friction forces against the plate from screw fixation and buttressing in metaphyseal and articular fractures, are limited in resisting applied loads versus locking fixation. Locking plates are recommended to use in situations with limited fixation options, osteoporotic bone, or need for fixed-angle support. Currently, most of the bone plates have increased with periarticular design and locking holes and the surgeon can decide the screw type, e.g. locking or nonlocking, depending on the fracture site and pattern.
1.3.2. Intramedullary nails
Intramedullary nails has been shown that there is limited interference of the device with the soft tissue around the fracture, hence, intramedullary nails may be superior in patients with chronic comorbidity, such as diabetes, neuropathy, and peripheral vascular disease because these patient populations are more prone to wound complications [29]. Intramedullary nails have become an attractive treatment due to their superior biomechanical advantages including higher stiffness for valgus and varus, weight and torsional loading [30,31]. And they allow stable fixation of simply diaphyseal fractures with early mobilization of joints, early ambulation, and weight-bearing of extremities. However, intramedullary nails do not contribute to satisfactory fracture reduction. Interlocking nailing devices provide better stability and rotational control, resulting in a reduced risk of nail migration and loss of fixation compared with unlocked nailing [32]. Intramedullary nails can be either reamed or non-reamed, where reaming is more beneficial for reduction. But stress occlusion of the fracture end can lead to destruction of local fracture integrity and lead to adverse clinical outcomes [33]. After the fracture end is reset, the fracture end micro-motion is provided to promote fracture healing, if the locking nail is fixed too firmly, the alignment may be poor, resulting in deformed rotation and broken nail [34].
1.3.3. Others (pins, wires, screws)
Wires (K-wires) and pins (S-pins) have various applications, for example, for bone traction, provisional fixation and definitive fracture fixation [35]. They are usually supplemented with other stabilization methods when used for fracture fixation, since the resistance to bending with wires is minimal. Wires and pins can provide provisional fixation for reconstruction of fractures while incurring minimal bone and soft tissue damage and leaving room for additional hardware placement. Planning pin placement is important to avoid the eventual permanent fixation devices, and if possible, wires and pins should be placed parallel to screws used for fracture compression. They may also be used as guide wires for cannulated screw fixation. Permanent fixation options include fractures in which loading is minimal or protected with other stabilization devices, such as external fixators, plates, and braces [36,37].
Bone screws are a basic part of internal fixation and can be used independently or in combination with particular types of implants [38,39]. Two basic types of screws are available for usage in bone of differing density, cortical screws which designed for compact diaphyseal bone, and cancellous screws which designed for the more trabecular.
It can be seen from Table.1 that bone plates are the most common implants in internal fixation [20]. To satisfy the bone healing requirements of the biomechanical microenvironment, the structure and materials of bone plates have gone through a long evolution.
Along with advances in the understanding of the factors that influence fracture healing, fracture fixation plate designs have experienced continuous innovation. The design philosophy of the bone plates can be classified into three categories: compression plates, limited-contact plates and biological fixation plates [19].
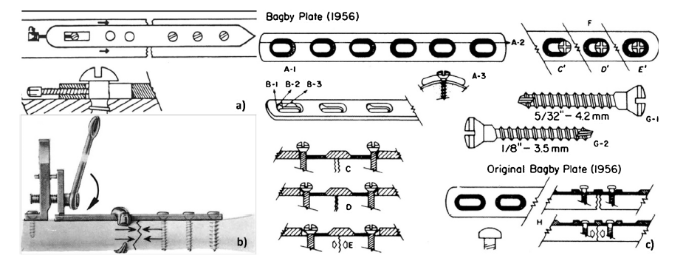
Before people realized the significance of micromotion on fracture healing, bone plates were designed to fix the ends of the fracture as stable as possible [40]. Following this principle, coapteur plates, tensioner plates and dynamic compression plates (DCPs) arose, which can be collectively called compression plates (Fig. 4). The advantages of the compression plate include low incidence of mal-union, stable internal fixation, and no need for external immobilization, thus allowing immediate movement of neighbouring joints [19]. However, compression plates also have obvious shortcomings: 1) fractures fixed by compression plate healed mainly by primary healing, which was a long and slow process, 2) microscopic fracture lines remained after the removal of the plate, which probably act as stress raisers and preferential sites for fatigue crack initiation, and 3) loss of bone mass occurred at the subcortical bone, leading to osteoporosis and secondary bone fracture [40].
Fig. 4. Bone plates design of (a) Coapteur plate, (b) Tensioner plate, (c) Dynamic compression plate (DCP). Reprinted from Ref. [
Perren et al. proposed that excessive contact between bone plate and cortical bone impeded blood flow and caused necrosis of the cortical bone under the plate, which was supposed to be the main cause of local osteoporosis [42]. The limited-contact plate (LCP) was developed based on this knowledge. However, Field et al. compared the actual contact area between DCP and LC-DCP with the cortical bone underneath the plate. It was found that there was essentially no significant difference between these two designs [43]. Jain et al. measured cortical blood flow with laser Doppler flowmetry of canine tibias fixed with a DCP or LC-DCP and produced results were consistent with those of Field et al. [44]. The biomechanical properties of the tibiae were also the same. Hence, it can be concluded that the LCP has no advantage in terms of fracture healing or restoration of cortical bone perfusion to devascularized cortex. Afterwards, point contact fixator (PC-Fixator) was developed, in which the contact area between the plate and cortical bone was decreased attributed to point contact. Tepic et al. investigated the therapeutic efficacy of a standardized oblique fracture of sheep tibia treated with DCP and PC-Fixator and found that PC-Fixator could help the tibia obtain faster recovery of mechanical function [45]. Haas et al. treated fractures of the forearm using PC-Fixator. Compared with the conventional plate, fracture fixation with PC-Fixator presented multiple advantages: easier operation, shorter healing time and less surgical complications [46]. Despite the advantages of the PC-Fix, osteoporosis, which occurred underneath the plate after long-term implantation, was still not solved.
Fracture fixation by conventional plates aims to give necessary mechanical stability to the fracture ends, and any micromotion is expected to be avoided. Unexpectedly, Goodship and Kenwright found that micromotion at the fracture ends could actually help accelerate fracture healing and decrease the rate of delayed union and non-union [47]. Gerber et al. proposed the concept of biological internal fixation [48]. This concept changed the traditional idea that mechanical stability should be the primary consideration to emphasize meeting the biological needs of fracture healing. Biological internal fixation encourages the formation of callus, while a less precise and indirect reduction will reduce operative trauma [40]. Fracture healing by stiff internal fixation is achieved by primary healing, while biological internal fixation focuses on the activation of secondary healing. In the condition of biological internal fixation, the fracture heals faster, and the healed bone tissue has better mechanical performance. Guided by this concept, Hans et al. designed plates that allowed micromotion in the axial direction [49]. The screw shank and the wall of the oval screw holes in the plate allowed compression of the fracture gap under loading and rebound after unloading. From the histologic examinations of experimental animals, it was found that earlier bridging between the fragments and more rapid healing than conventional plates were achieved. Minimally invasive percutaneous osteosynthesis (MIPO) was also developed based on this concept [50]. Micromotion in the axial direction was allowed for the fracture ends when loading was applied to bone fixed by MIPO. Micromotion helped to promote callus formation and accelerate fracture healing. The contact area between the plate and the cortical bone is almost negligible, so it does not interfere with the blood flow of the bone underneath the plate.
Overall, biological internal fixation is an effective way to improve bone healing by activation of secondary healing, which has been a great advancement for the treatment of fractures in comparison with traditional plates [51,52]. However, after fracture healing, the plates and screws will remain in the body unless they are required for removal through a secondary operation, which will cause a series of adverse effects, such as inflammation or allergies, due to corrosion and wear of the plates [53]. Even if the plate was removed by a secondary operation, the remaining screw holes may also serve as stress raisers and preferential sites resulting in fatigue cracks. Therefore, it still remains an urgent problem for orthopaedic surgeons to seek a more ideal way of internal fracture fixation [22,54,55].
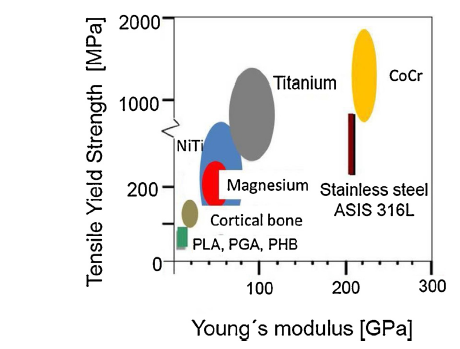
Micromotion is considered a favourable factor in promoting fracture healing, but this process can also be impeded by excessive interfragmentary instability [56]. Therefore, it is the fundamental function of fixation plates to provide necessary stability to the fracture ends, which puts forward a high demand to the mechanical properties of the plates, especially when the plates are used in fracture fixation at load-bearing bones, such as the tibia and femur [57]. Among various biomaterials, metallic biomaterials possess excellent comprehensive mechanical properties, including high strength, high toughness and good process ability. Hence, metallic biomaterials are the most commonly used for manufacture of bone plates [58]. The earliest literature on metallic bone plates was dated back to 1895. The plates were made of vanadium steel, but they were abandoned due to severe corrosion in the human physiological environment [59]. At present, the bone plates commonly used in the clinic are mainly made of stainless steel and titanium alloy [[60], [61], [62]]. In recent years, plates made of resorbable polymer are also coming into view [[63], [64], [65]]. Fig. 5 shows the mechanical properties of cortical bone and materials used for orthopaedic implants.
Fig. 5. Mechanical properties of cortical bone and materials for orthopaedic implants.
Stainless steel used for manufacture of bone plates began in the 1930s [66]. Stainless steel is the generic name for a number of iron-based alloys that contain a high percentage of chromium (11-30 wt%) and varying amounts of nickel [67]. Stainless steel can be grouped into four groups based on their characteristic microstructure: martensitic, ferritic, austenitic, and duplex (austenitic plus ferritic) [68]. Among them, only austenitic stainless steels, especially type 316L, are used for implants due to their best corrosion resistance, better fatigue strength, more ductility, better machinability and non-magnetism [69]. Table 2 lists the composition of 316L (ASMT F138) stainless steel and its variants. 316L austenitic stainless steel possesses excellent comprehensive mechanical properties (Table 3). These have widely been used in the manufacture of bone plates.
Table 2 Compositions (wt%) of 316L stainless steel (ASTM F138) and variants [
| ASTM code/UNS No of stainless steels | Cr | Ni | Mo | Mn | Si | Cu | N | C | P | S |
|---|---|---|---|---|---|---|---|---|---|---|
| F138/S31673 | 17.00-19.00 | 13.00-15.00 | 2.25-3.00 | 2.00 | 0.75 | 0.50 | 0.10 | 0.030 | 0.025 | 0.010 |
| F1314/S20910 | 20.50-23.50 | 11.50-13.50 | 4.00-6.00 | 2.00-3.00 | 0.75 | 0.50 | 0.20-0.40 | 0.030 | 0.025 | 0.010 |
| F1586/S31675 (Orthinox) | 19.50-22.00 | 9.00-11.00 | 2.00-4.25 | 2.00-3.00 | 0.75 | 0.25 | 0.25-0.50 | 0.08 | 0.025 | 0.010 |
| F2229/S29108 | 19.00-23.00 | 0.10 | 21.00-24.00 | 0.50-1.50 | 0.75 | 0.25 | >0.90 | 0.08 | 0.03 | 0.010 |
Table 3 Mechanical properties of 316L stainless steel [
| Young’s modulus (GPa) | Ultimate tensile strength (MPa) | Fatigue strength (MPa, 107 cycles) |
|---|---|---|
| 193 | 540-1000 | 240-480 |
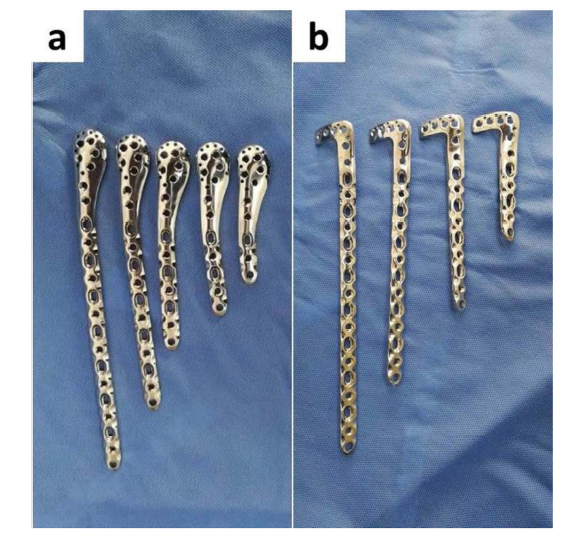
316L austenitic stainless steel plates (Fig. 6) provide sufficient fixation for the fracture fragments. However, the Young’s modulus (approximately 193 GPa) of stainless steel is much higher than that of cortical bone (approximately 10-30 GPa), which leads to a severe stress shielding effect and slow healing rate due to the lack of mechanical stimulus [70]. The human body presents an aggressive environment for stainless steel due to the presence of chloride ions and proteins. Furthermore, the internal partial pressure of oxygen is about one-quarter of the atmospheric oxygen pressure. While less reactive in terms of oxidation, lower oxygen actually accelerates corrosion of metallic implants by slowing down the formation of protective passive oxide films on the metal surfaces [71]. There are mainly two kinds of corrosion of stainless steels in body fluid: pitting corrosion and crevice corrosion; in particular, the latter is the primary cause leading to fixation instability of stainless steel plates [72]. In addition to not satisfied corrosion resistance, 316L stainless steel also has a number of other long-term issues, including stress corrosion cracking, poor wear resistance, and the toxicity and carcinogenicity of the released nickel (Ni) and chromium (Cr) ions [73,74]. Research on the development of Ni-free stainless steels is in progress [75,76]. A large amount of nitrogen (N), which is an austenite stabilizing element, is added instead of Ni (also an austenite stabilizing element) to make Ni-free stainless steel. The addition of N in 316L can also increase mechanical strength as well as enhance resistance to pitting and crevice corrosion [77]. Ren et al. developed a kind of high-nitrogen nickel-free stainless steel (HNNFSS), which possesses excellent mechanical properties, corrosion resistance and biocompatibility. In particular, its strength is twice that of the conventional 316L stainless steel. The resistances to bending, tension and compression of HNNFSS plate are all better than those of 316L plate when its thickness is thinned to less than 18% of the original size [77].
Fig. 6. 316L stainless steel bone plates used for (a) humeral fracture and (b) tibial fracture.
The earliest application of titanium alloy used as orthopaedic implant material dated back to 1940s [79]. Based on the characteristic microstructure, titanium alloys are categorized into four groups: α alloy, near-α alloy, α + β alloy and β alloy [79]. Among them, the application of α alloy and near-α alloy as orthopaedic implant materials is confined in scope due to their poor mechanical performance. Most of the biomedical titanium alloys belong to the α + β or metastable β type. The strength of these two kinds of titanium alloys could be enhanced to meet the load bearing request for plate materials by solid solution and aging treatment [80].
Compared with stainless steels, titanium alloys present lower modulus, higher specific strength, superior biocompatibility and enhanced corrosion resistance [79]. These attractive properties drove their wide applications in the clinic as bone plate materials. TiO2 passive film tends to form on the surface of titanium alloys, which has a significantly protective effect on the titanium alloy substrate against body fluids [81]. If damaged, this passive film can reform immediately at body temperature and in physiological fluid. This feature ensures excellent corrosion resistance of Ti-based alloy implants in vivo [82]. There is little or no reaction with surrounding tissues for the titanium alloy plates [83]. Once a plate made of stainless steel is implanted into the body, a capsule naturally forms around the plate, which is one of the reasons of implant loosening [84]. Interestingly, titanium alloys are not recognized by tissues as a foreign body in vivo, and they have excellent affinity with bones [67].
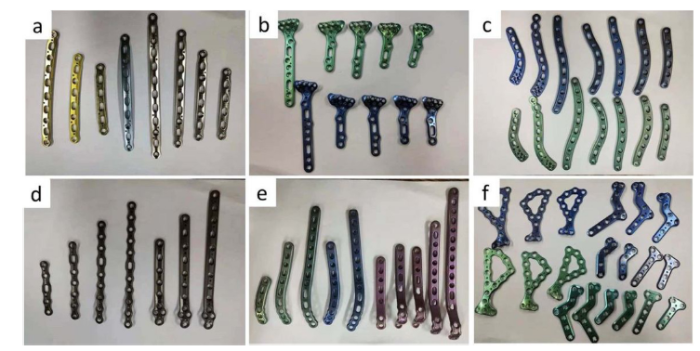
The mechanical properties of Ti-based alloys used as plate materials are presented in Table 4. Ti-6Al-4V ELI (extra low interstitial) alloy is the most commonly used titanium alloy for bone plate (Fig. 7) [85,86]. Ti-6Al-4V alloy was originally developed for aerospace applications, and its high corrosion resistance and excellent biocompatibility led to its entry into the biomedical field [79]. However, Al and V ions released from Ti-6Al-4V alloy are found to be associated with long-term health problems. Furthermore, titanium has poor shear strength, making it less desirable for bone plates. Ti-based alloys that have high friction coefficient can lead to formation of wear debris may result in an inflammatory reaction causing pain and loosening of plates due to osteolysis [79]. The development of second generation of titanium alloy was started in the 1990s [87]. Element Al and V were eliminated in the second generation of titanium alloys by other β phase-stabilized elements with better biocompatibility, such as Nb, Zr, Mo and Ta [66,88]. The second generation of titanium alloys are characterized by single β phase. They possess better biocompatibility and corrosion resistance. Furthermore, compared to titanium alloy with α + β duplex phases, the elastic modulus of titanium alloys with single β phase is greatly reduced down to 55-85 GPa without sacrificing their mechanical strength [79]. A closer gap in the elastic modulus between plate and its adjacent bone will greatly reduce the rate of secondary fracture induced by stress shielding. It is a trend that traditional plates will be replaced by plates made of β phase titanium alloys. However, potential accidents, including fracture and loosening of the plates, due to poor wear resistance and fatigue resistance are always intricate problems for titanium alloys used as plate materials [67].
Table 4 Mechanical properties of titanium and titanium alloys used as bone plate materials [
| Material | Standard | Modulus (GPa) | Tensile strength (MPa) | Alloy type | Smooth fatigue limit at 107 cycles (MPa) | Notch fatigue limit at 107 cycles (MPa) |
|---|---|---|---|---|---|---|
| First generation Ti-based medical metallic material (1950-1990) | ||||||
| Commercially pure Ti | ASTM 1341 | 110 | 240-550 | α | 88-413 | |
| Ti-6Al-4V ELI wrought | ASTM F136 | 110 | 860-965 | α + β | 500 | 290 |
| Ti-6Al-4V ELI Standard grade | ASTM F1472 | 112 | 895-930 | α + β | ||
| Ti-6Al-7Nb Wrought | ASTM F1295 | 110 | 900-1050 | α + β | 500-600 | |
| Ti-5Al-2.5Fe | - | 110 | 1020 | α + β | 580 | 300 |
| Second generation biomaterials (1990-till date) | ||||||
| Ti-13Nb-13Zr Wrought | ASTM F1713 | 79-84 | 973-1037 | Metastabe β | 500 | 335 |
| Ti-12Mo-6Zr-2Fe (TMZF) | ASTM F1813 | 74-85 | 1060-1100 | β | 525 | 410 |
| Ti-35Nb-7Zr-5Ta (TNZT) | - | 55 | 596 | β | 265 | |
| Ti-29Nb-13Ta-4.6Zr | - | 65 | 911 | β | ||
| Ti-35Nb-5Ta-7Zr-0.40 (TNZTO) | - | 66 | 1010 | β | 450 | |
| Ti-15Mo-5Zr-3Al | - | 82 | β | |||
| Ti-Mo | ASTM F2066 | β | ||||
Fig. 7. Ti6Al4V bone plates. (a) The ulna bone plate; (b) The radial bone plate; (c) The clavicular bone plate; (d) The ulna olecranon bone plate; (e) The ankle bone plate; (f) The calcaneal bone plate.
Co-Cr-Mo alloy and Co-Ni-Cr-Mo alloy are two typical medical Co-Cr alloys. The as cast Co-Cr-Mo alloy has been used as a medical metal material for decades. In the early stage, it was mainly used as dental material. Recently, it has been widely used in the field of artificial joint. As a medical metal material, Co-Ni-Cr-Mo alloy has been used for a relatively short time and is mainly used to make the shank of knee or hip joint prostheses that need to bear a large load [89].
American Society for Testing Material (ASTM) has recommended four Co-Cr alloys for medical metal materials including cast Co-Ni-Cr-Mo alloy, wrought Co-Cr-W-Ni alloy, wrought Co-Ni-Cr-Mo alloy, and wrought Co-Ni-Cr-Mo-W-Fe alloy. At present, cast CoCrMo alloy and wrought Co-Ni-Cr-Mo alloy are widely used. For these two alloys, the content of Co can be up to 65%, and the alloy element Mo can significantly refine the grain size of the alloy. Cr, on the one hand, can play the role of solid solution strengthening, and on the other hand, can significantly improve the corrosion resistance of the alloy [90].
The wrought Co-Ni-Cr-Mo alloy and the cast Co-Cr-Mo alloy had similar wear resistance (both had a wear rate of 0.14 mm/year in the acetabular cup wear test). Wrought Co-Ni-Cr-Mo alloy has high tensile strength and fatigue resistance. The elastic modulus of Co-Cr alloy is between 220-234 GPa, which is far above that of the bone tissue [91]. It can be expected that stress shielding will not be avoidable, which will impair the healing of the bone fracture. In addition, the results of in vitro experiments showed that Co particles had a toxic effect on osteoclasts, and they also inhibited the synthesis of type I collagen, osteocalcin and alkaline phosphatase. And the extractive liquid of Co and Ni had significant cytotoxicity, significantly reduced the survival rate of cells, and the extractive liquid of Cr also had cytotoxicity [92]. Therefore, due to wear, corrosion and release of metal products, CoCr alloys have adverse effects on the surrounding bone tissues. Furthermore, poor fabricability and high costs also make Co-Cr alloys currently unsuitable for broad use as bone plates.
In addition to the Ti-based alloys, NiTi alloy as a famous shape-memory alloy, which is considered to have broad application prospects in the medical field [67]. NiTi alloy has good workability and corrosion resistance [93]. The young's modulus of NiTi alloy is between 30-50 GPa [94], which is even closer to cortical bone than that of titanium alloy, and the yield strength and tensile strength of NiTi alloy reach the same level as that of stainless steel. The human body provides a relatively aggressive environment, which requires relatively high corrosion resistance of long-term implant materials [95]. A large number of in vitro and in vivo experimental results showed that the corrosion resistance of NiTi shape memory alloy was better than 316L stainless steel and CoCrMos alloy, but weaker than pure titanium [67]. However, NiTi alloy contains high concentration of Ni element (about 50 at%). For this reason, clinical trials of NiTi alloy in vivo have mostly focused on implants with small-size, such as cardiovascular stents, fixation staples [96], clips [97] and clamps [98]. According to Dai a NiTi shape memory alloy staple was first used inside the human body in 1981. NiTi alloy staples and clamps were used in comminute fractures of short tubular bone, for fixation of mandibular fractures, metatarsal osteotomies, anterior cervical decompression and fusion, fixation of small bone fragments, and for several other cursory applications [98]. No conclusive and convincing experimental data have been reported on the long-term existence and biosafety of large NiTi alloy implants in vivo. The bone plate in the body bears the friction and wear with screws, surrounding bone tissue, and body fluids corrosion etc., which will lead to more Ni elements released into the body that is bound to have adverse effects on human health. At the same time, from the point of view of fatigue strength, NiTi shape memory alloy is also weaker than stainless steel, Co or Ti alloy [67]. Therefore, compared with the traditional stainless steel or titanium alloy, NiTi alloy does not show better performance when used as the bone plate material. Currently, there is no report on the application of NiTi alloy as the bone plate material as it is not recommended to be used as implant materials for in vivo applications.
The Young’s modulus of metallic materials are approximately 5-10 times that of skeletal tissues. Therefore, stress shielding induced by traditional metallic plates is always unavoidable. Polymers have been used in many engineering applications due to their light weight and easy formability [99]. In the recent decades, polymeric materials have also been widely studied as orthopaedic implant materials [100]. Table 5 shows the mechanical properties of polymers and their composites that are extensively used and investigated as orthopaedic implant materials. Their elastic modulus values are found between 0.5 and 10 GPa, close to or even lower than that of skeletal tissues [101]. It is expected that plates made of polymeric materials does not induce stress shielding. Polymeric materials show lower interference with computed tomography (CT) and magnetic resonance imaging (MRI), which contributes to monitoring fracture healing using medical imaging modalities [102]. In addition, some polymeric materials, such as PLA, PLLA and D-PLA, can be degraded in the body, therefore, implant removal surgery can be avoided after fracture healing [99].
Table 5 Mechanical properties of different synthetic polymers studied as bone plate biomaterials [
| Materials | Elastic modulus (GPa) | Tensile strength (MPa) |
|---|---|---|
| HDPE | 0.88 | 35 |
| PTFE | 0.50 | 28 |
| PA | 2.10 | 67 |
| PMMA | 2.55 | 59 |
| PET | 2.85 | 61 |
| PEEK | 8.30 | 139 |
| PS | 2.65 | 75 |
| PLA | 2.40 | 60 |
On the other hand, the main limitations of polymer plates are associated with their inferior mechanical properties [64]. They are weaker than conventional titanium alloy plates, leading to low confidence levels regarding the stability of reduced fractures at load-bearing skeletal sites [103]. It was however reported that polymeric materials are safe, effective and sufficiently flexible when they were used at many maxillofacial bony surgical sites. Therefore, they are now much appreciated in oral and maxillofacial osteosynthetic applications [104].
Bone tissue is a composite of organic materials (mainly collagen) and ceramic materials (hydroxyapatite) [105]. Inspired by this composition, material scientists thought of adding strength phases, such as ceramics, metals and fibers, to form polymer matrix composite materials with increased mechanical properties, thereby making them meet the load demands [106]. Advantages of the polymer matrix composites lie in their adjustable mechanical performance by multivariable factors according to different applications. These variables include the types of matrix, the types of strengthening phases, the particle size distribution of strengthening phases, and the quantity of strengthening phases [107,108]. Zahra et al. designed a kind of plate made of carbon fibre/flax/epoxy resin composite materials. The bending strength and tensile strength of this composite are 510.6 MPa and 399.8 MPa, respectively, which are close to metallic materials. Its bending modulus and tensile modulus are 41.7 GPa and 57.4 GPa, respectively, which are closer to those of cortical bone compared with traditional titanium alloys. Therefore, it is considered a good candidate as bone plate material [109].
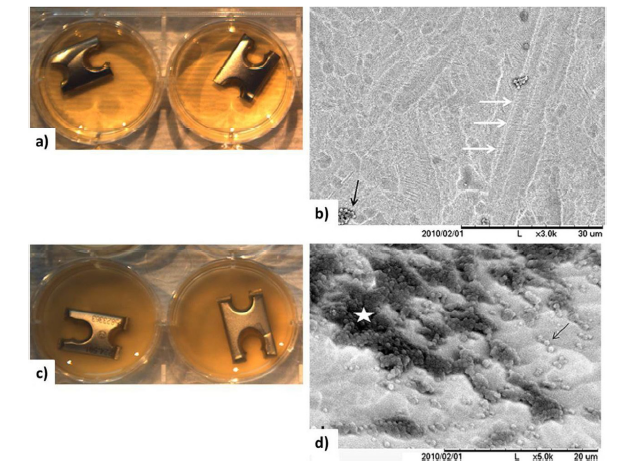
Infection caused by orthopedic implants is an important reason for the failure of internal fixation in fracture repair [110]. Infections result in higher morbidity, mortality, and treatment costs. Even after many precautions have been taken to prevent infection, the risk of bacterial infection of the plate remains as high as 5%-10%, and the risk of infection after an open fracture fixation is even higher [111,112]. The colonization of bacteria and the formation of biofilm on the surface of the bone plate are the main causes of fracture site infection, which is difficult to be completely eradicated [113,114]. To solve this problem, a wide range of local debridement, and in combination with systemic and targeting of antibacterial treatment is required. However, these methods can only ease the bacterial infection to a certain extent [115]. So how to prevent infections caused by bone plate is an urgent issue or task of materials experts and clinical doctors. The existing researches on bone plate surface modification are mainly focused in this clinically relevant field. The studies reported in the literature on improving the antibacterial properties of the surface of bone grafting plates were carried out from the following three aspects: formation hydrophobic surface on the bone plates [110], coating the surface of the bone plates with antibiotics [116], coating the surface of the bone plates with antibacterial elements (silver, copper, etc.) [117]. For example, Schaer et al. [110] coated the surface of the bone plate with hydrophobic polycation (N,N,dodecyl,methyl-PEI). As shown in Fig.8, they studied the antibacterial properties of hydrophobic polycation to staphylococcus aureus. The results showed that very few coalescing planktonic cocci were observed on the surface of the hydrophobic polycation coated samples. However, the formation of a large number of bacterial membranes was observed on the surface of the uncoated sample, which indicates that hydrophobic polycation can help the bone plate resist the colonization and the biofilm formation of staphylococcus aureus on its surface. The in vivo experiments results showed that the bone plate coated with hydrophobic polycation not only inhibited the occurrence of infection, but also accelerated the healing of fracture. They attributed the anti-infection effect of hydrophobic polycation to its destruction role to the cell membrane of bacterials. The cell membrane fragments trig immune responses of the organism, thus eliminating it before the forming the bacterial biofilm. Stewart et al. [116] coated titanium bone plate using vancomycin by the way of covalent bonding. In vitro experiment results showed that cell membranes of bacteria were damaged on vancomycin coated bone plate. In vivo experiment results showed that vancomycin coating can greatly decrease the incidence of fracture site infection and protect the bone fracture healing from the adverse effects of staphylococcus aureus. So it was expected that binding of vancomycin to the surface of bone plates held great promise in helping to reduce protracted and recalcitrant implant-associated with the recovery of patients in orthopaedic. It is a common knowledge that silver nanoparticles have antibacterial properties. As bacteria become more and more resistant to antibiotics, people begin to consider using silver nanoparticles as an alternative to antibiotics to resist infection. Soloviev et al. [117] prepared nanometer silver coating on the surface of stainless steel plate by the sonochemical method. They studied the effects of reaction conditions on the performance of the nano silver coatings. It was found that when the distance of the stainless steel plate from the sonicator tip was 1 cm, a homogeneous monolayer coating of silver nanoparticles with an average particle size of 40 nm was obtained on the surface of the stainless steel bone pate. They expected that the silver nanoparticle layer could inhibit the bacteria colonization and bacteria biofilm formation on the surface of the bone plate, thus reducing the incidence of infection related to the bone plate, which remains to be verified by further in vivo and in vitro experiments.
Fig. 8. Comparison between N,N-dodecyl,methyl-PEI-coated (a, b) and uncoated (c, d) stainless steel plate chips obtained in parallel during the surgical implantation to independently validate the bactericidal activity applied to hardware in the operating theater. Wells containing coated plate chips remained clear (a) and devoid of biofilm when analyzed under SEM (b). In contrast, uncoated plate chips presented with turbid wells consistent with bacterial growth (c) and massive biofilm formation (d; biofilm (*), coalescing S. aureus cocci (arrow)). Reprinted from Ref. [
Due to demographic changes and intense exercises, the population suffering from refractory fractures such as osteoporosis fractures and comminuted fractures are increasing, which poses a challenge to traditional bone plates. Therefore, optimal fracture treatments are desirable. For conventional one plates, their main function is to provide mechanical fixation for the fracture ends during fracture healing. Then, by virtue of the body’s physiological functions, the fracture experiences bridging and bone remodeling, ultimately achieving the goal of functional recovery by way of primary healing or mostly secondary healing. There are three major problems with conventional bone plates for internal fixation of fracture: (1) loosening tends to occur after long-term implantation, and a second operation for implant removal is needed; (2) stress shielding originating from a mismatch of Young’s modulus leads to the risk of second fracture; (3) there are high risks of delayed union or non-union in case of complicated fractures, such as comminuted fractures and osteoporotic fractures.
Traditional bone plates are mostly made of bio-inert materials. Along with the development of biomaterials, Hench et al. put forward the concept of the third generation of biomaterials, which pointed out that these biomaterials should be designed to stimulate specific cellular responses at the molecular level [118]. As a basic discipline, the development of material science can promote a qualitative leap in many fields. As the most commonly used implant in the field of orthopaedics, bone plates are also in an important period for development. Here, we envisage a new concept of bone plate, which should have the following characteristics: (1) providing reliable fixation for the fracture ends, (2) avoiding stress shielding, (3) eliminating the need for a second operation due to biodegradation of implant after implantation over time, (4) activating biological functions related to fracture healing and accelerating fracture healing attributed to the anabolic effects of the degraded products of the implants.
To realize this new concept of the bone plates, many attempts have been made by using biomaterial strategies [119]. In the process of fracture healing, the biological behaviors of the MSCs adjacent to the fracture site, including migration, proliferation, differentiation and biological factor release, play a crucial role [6,120,121]. Research has focused on promoting these behaviors of the MSCs to enhance fracture healing from two perspectives below [22,54,122].
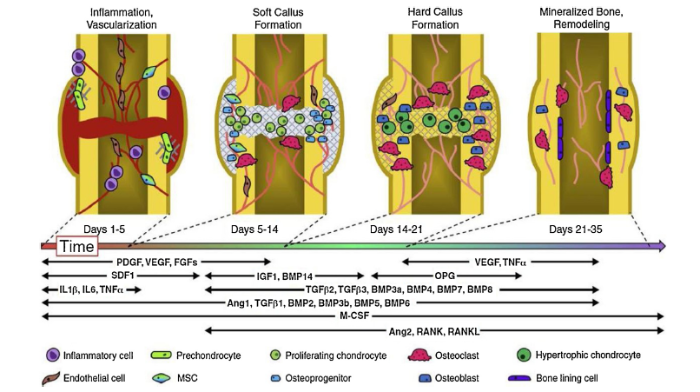
The spatiotemporal cascade of multiple endogenous factors controlling normal bone regeneration during fracture repair is summarized in Fig. 9. As shown in Table 6, some drugs, biological factors and metallic ions possess the efficacy to promote fracture healing.. As shown in Table 6, some drugs, biological factors and metallic ions possess the efficacy to promote fracture healing.
Fig. 9. A spatiotemporal cascade of multiple endogenous factors controls normal bone regeneration during fracture repair in four stages. PDGF: platelet derived growth factor; VEGF: vascular endothelial growth factor; FGF: fibroblast growth factor; TNF: tumor necrosis factor; SDF: stormal cell-derived factor; IGF: insulin-like growth factor; BMP: bone morphogenetic protein; OPG: osteoprotegerin; IL: interleukin; TGF: transforming growth factor; Ang: angiopoietin; M-CSF: macrophage colony stimulating factor; RANK: receptor activator of nuclear factor κB; RANKL: RANK-ligand. Reprinted from Ref. [
Table 6 Effects of biological factors, drugs and metallic ions for fracture healing [6,79,[
| Category | Designation | Efficacy | Outcomes |
|---|---|---|---|
| Inflammatory Growth Factors | TNF-α | Promote bone resorption by enhancing osteoclast differentiation and activity. | |
| ILs | IL-1: stimulate IL-6 secretion in osteoblasts and promote the formation of primary callus and angiogenesis at the injured site. IL-6: essential for the early phases of fracture healing and can promote monocytes differentiation to osteoclasts and also influence MSCs to the pre-osteoblast fate; recruit monocytes/macrophages. IL-11 and IL-17: promote bone resorption by enhancing osteoclast differentiation and activity. IL-10 and IL-13: inhibite bone resorption by enhancing osteoclast differentiation and activity. | IL-6: Significantly increased BMP-2/ACSb) -induced bone mass via IL-6 injection. IL-3: Enhanced bone formation. | |
| Angiogenic Growth Factors | VEGF | Regulates the recruitment, survival and activity of endothelial cells, osteoblasts and osteoclasts; mediated capillary invasion | Increase percent calcified callus and increased vascu- larity in soft tissue surrounding fracture; |
| PDGFs | Targets MSCs to promote proliferation and angiogenesis, connector between the cellular components and contributors of the osteoblast differentiation process, | Increased callus formation, increased rate of union. | |
| FGFs | Regulate cell migration, proliferation, and differentiation. stimulates capillary growth by modulating endothelial cell fate as well as MSCs. | Faster callus formation of fracture and higher percentages of fracture union. | |
| Osteogenic Growth Factors | BMPs | Stem cell commitment of chondrogenic and osteogenic lineages, chondrocyte hypertophy and coupled remodelling, participate in the regulation of osteoblast lineage-specific differentiation and later bone formation, osteogenic activity in bone formation in ectopic and orthotopic sites | Increased callus size, increase stiffness |
| Systemic Factors | PTH | Chondrocyte and osteoblast proliferation, delayed chondrocyte hypertophy, increased coupled remodelling | Increased callus size, bone mass and mineral content, increase stiffness and strength. |
| Calcitonin | Reduce blood calcium and promotes bone formation via inhibiting bone removal by osteoclasts and enhance bone generation by osteoblasts. | ||
| Drugs | Alendronate | Inhibit osteoclast-mediated bone resorption and also expedite the bone-remodeling activity of osteoblasts | Increased callus formation, bone mass. |
| Trace elements | Mg | Stimulate the dorsal root ganglion (DRG), leading to the rise of calcitonin gene related peptide (CGRP) expression. Next, the rise of CREG expression enhanced the osteogenesis differentiation of the MSCs, which promote the formation of callus around the Mg implant. | Increased callus size, bone mass and mineral content, increase stiffness and strength. |
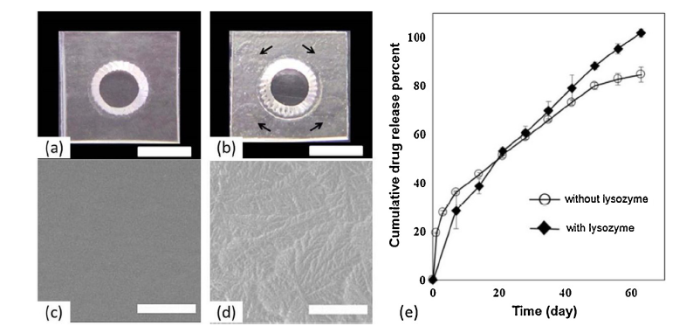
As shown in Fig. 10, Hur et al. prepared a bone plate enabling local and sustained release of alendronate, which is a drug known to inhibit osteoclast-mediated bone resorption and to expedite the bone-remodeling activity of osteoblasts [128]. The bone plate was made of trimethylene carbonate, polylactide and polyglycolide, and was coated with photo-crosslinked 4-azidobenzoic acid-modified chitosan loaded with alendronate (AL-Az-CH_P). This plate could be degraded in body fluid without requiring implant removal surgery. It was found that the drug could be released from the plate surface coating for approximately 63 days in a sustained manner, maintaining a therapeutically effective drug level. When this alendronate-delivery plate was fixed on a calvarial critical size defect in vivo, a significantly higher volume of newly formed bone was observed than on bone with the plate without the drug. As for growth factors, which have shown great potential in bone regeneration, their short biological half-life in physiological conditions due to rapid degradation and deactivation, high cost and severe side effects have limited their clinical application. Lowering the dosage and optimizing the treatment efficacy and safety of treatment are important [125].
Fig. 10. Optical images of the plate samples (a) without and (b) with the coating. The arrows indicate the locations of the coatings. The scale bars represent 3 mm. Scanning electron micrographs of the surfaces (A) without and (B, C) with the coating on the AL-Az-CH_P. The scale bars represent (A, B) 100 μm; (e) In vitro drug release profiles of the AL-Az-CH_P with and without lysozyme. Reprinted from Ref. [
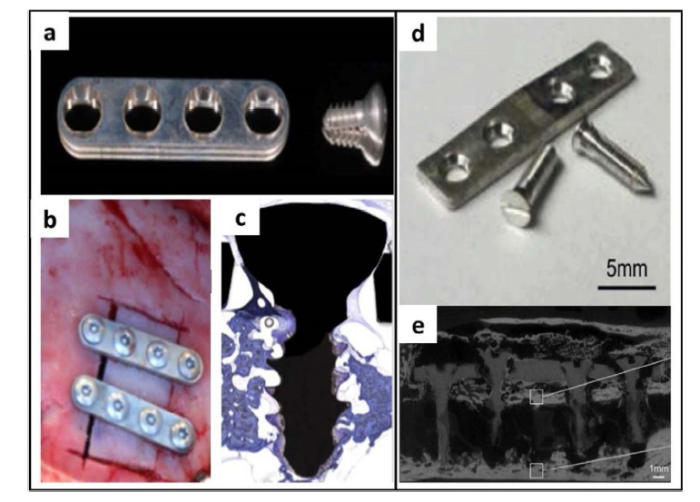
Among the newly developed biomaterials, magnesium (Mg) and its alloys present excellent comprehensive mechanical properties and biocompatibility. There was significant research interest in using Mg-based alloy bone plate for the treatment of bone fracture [78]. The Young’s modulus of Mg is approximately 45 GPa, which is close to that of cortical bone, so it is expected that stress shielding can be significantly reduced [129]. Mg is degradable in physiological fluids, and it has been widely reported that Mg ions, the degradation product of Mg, is beneficial to bone fracture healing [130]. Therefore, it is expected that Mg is a promising biomaterial to meet the requirements of ideal bone plates. With low degradation rate and no concern of releasing other biologically safe alloying elements, pure Mg is considered as one of the alternative materials for degradable bone plate. Naujokat et al. [131] studied plates and screws made of pure Mg for internal fixation of a cranio-osteoplasty in nine minipigs (Fig.11(a-c)). The results showed that Mg plates lead to undisturbed bone healing in all cases and biocompatibility of Mg with bone and soft tissue is sufficient. So it was confirmed that Mg plates osteosynthesis was suitable for internal fixation procedures. As shown in Fig. 11(d-e), Chaya et al. [55] studied the treatment effect of pure Mg plates and screws for the fixation of rabbit ulna fractures. New bone formation was observed around the degrading Mg implants. Fracture healing was observed by 8 weeks and maturation or remodeling after 16 weeks. Bending tests revealed that there was no difference in the flexural load between the healed ulnae with Mg implants and the intact ulnae, suggesting that Mg implants provided sufficient stability to facilitate fracture healing through degraded Mg ions to stimulate new bone formation [55].
Fig. 11. Pure Mg plates and screws used for the bone fracture fixation. (a-c) Osteosynthesis of a cranio-osteoplasty with a biodegradable pure magnesium plate system in miniature pigs; (d-e) Fixation of a rabbit ulna fracture with pure Mg fixation plates and screws. Reprinted from Ref. [
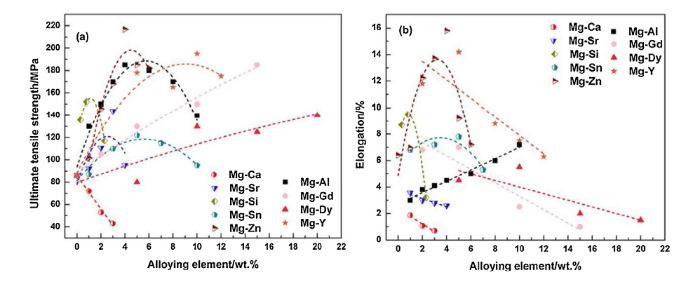
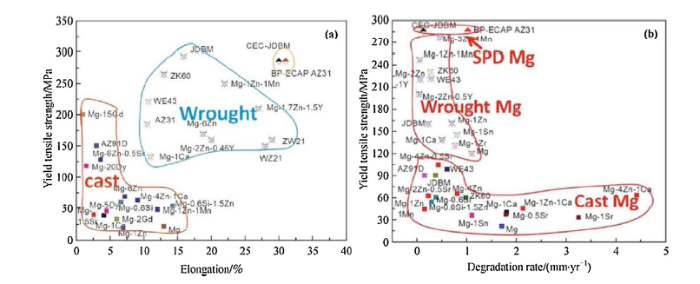
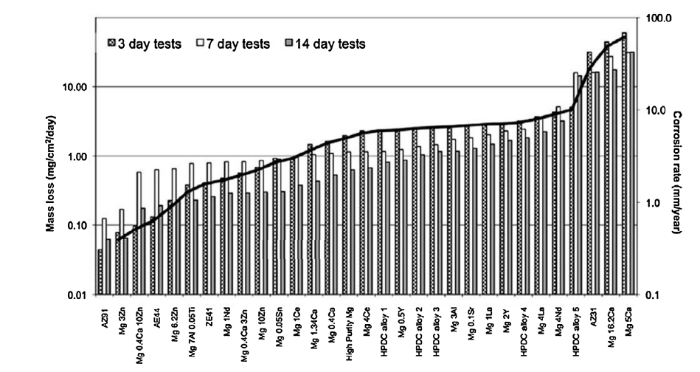
However, relative low strength is observed for pure Mg even after processing (the yield tensile strength is 21 MPa for as-cast Mg, 90-105 MPa for as-extruded Mg, and 115-140 MPa for as-rolled Mg) [133]. Erinc et al. [134] proposed specific mechanical and corrosion requirements for biomaterials purposed for bone fixtures: the corrosion rate needs to be less than 0.5 mm year-1 in simulated body fluid at 37 °C, the strength higher than 200 MPa and the elongation greater than 10%. Therefore, many studies have been conducted to improve the mechanical properties of Mg-based metallic materials including alloying, heat treatment and plastic deformation. As shown in Fig.12, Zheng et al. summarized the effects of adding different amount of alloying elements on the mechanical properties of Mg-based metallic materials [132]. The ultimate tensile strength and elongation of the as-cast Mg-zinc alloys significantly increased with increasing zinc contents up to 4 wt.%. And zinc is one of the essential trace elements for human body. Therefore, it seems to be that Mg-Zn alloys are promising materials for the bone plate. Gu et al. [135] studied the effects of plastic deformation on the mechanical properties and degradation behaviors of Mg-based metallic materials. It can be seen that both mechanical properties and corrosion resistance of the Mg-based metallic materials were improved (Fig.13). Zhang et al. [136] developed a new kind of Mg-Nd-Zn-Zr alloy. After extrusion and cyclic extrusion and compression (CEC) treatment, the Mg-Nd-Zn-Zr alloy exhibited yield strength of 300 MPa, elongation of 30%. However, the degradation rate of the E-CEC treated Mg-Nd-Zn-Zr alloy was 1-1.5 mm/year, which is higher than that (0.5 mm/year) as proposed by Erinc [134]. Xin et al. [137] summarized that degradation rates of various magnesium alloys in MEM solution (Fig. 14). It can be seen that degradation rates of most of the Mg alloys are higher than 0.5 mm/year. The rapid degradation rate may lead to the mismatch between the fracture healing rate and the decay of mechanical properties of the bone plate, which may lead to the loss of mechanical integrity of the bone plate before the fracture site recovers sufficient mechanical properties, leading to secondary fracture. Therefore, it is necessary to reduce the degradation rate of Mg alloys as much as possible. Various surface modification methods have been studied to improve the corrosion resistance of Mg alloys, including fluorine treatment, micro-arc oxidation, biomimetic deposition, electrodeposition and polymer coating [132]. Niu et al. [138] studied the effect of CaP coating on Mg alloy bone plate when it was used to treat tibia fracture of a rabbit (Fig. 15(a-g)). The result showed that more bony calluses formed around the Mg alloy plate, implying the efficacy of Mg ions in promoting fracture healing. The degradation rate was reduced obviously by the CaP coating and less gas was produced from CaP coated Mg-based bone plates and screws in early stage of the implantation, and at least 10 weeks degradation time was prolonged by the CaP coating [138]. It was reported that the micro-arc oxidation (MAO) method has the most significant improvement on the corrosion resistance of Mg-based metallic meterials [139]. Furthermore, the adhesion strength between the MAO coating and the Mg matrix is high, so it is expected to be applied to improve the corrosion resistance of Mg-based bone plate. Wu et al. [140] fabricated a microarc oxidation coatings contained Ca, P, Si on AZ31 Mg plate to investigate the in vivo corrosion degradation of the implants and bone fracture healing response using a 3 mm width bone fracture defect model (Fig. 15(h-k)). The in vivo studies indicated that the released Mg2+ promoted new bone formation. Both the in vitro electrochemical tests and in vivo degradation indicated that the corrosion resistance of the Mg implants was improved by the MAO coatings.
Fig. 12. Summary of (a) ultimate tensile strength, (b) elongation and for binary Mg-X alloys in the as-cast state as a function of alloying element content. Reprinted from Ref. [
Fig. 13. (a) Mechanical properties and (b) degradation rate of cast and wrought magnesium alloys in Hank’s solution at 37 °C. Reprinted from Ref. [
Fig. 14. Degradation rates determined from various magnesium alloy in MEM solution. Reprinted from Ref. [
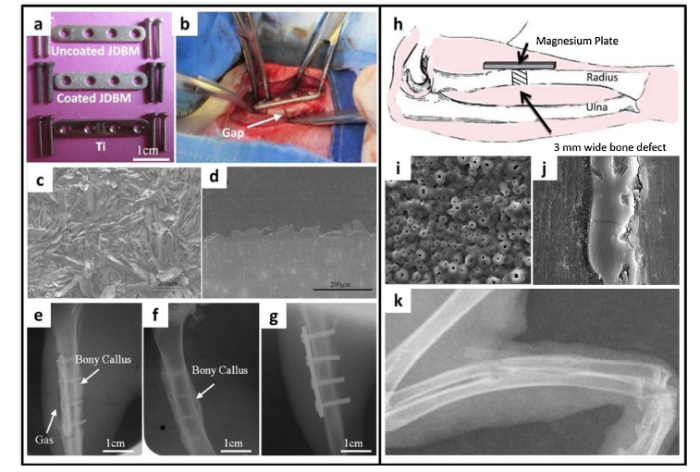
Fig. 15. Bone fracture fixation by Mg-Nd-Zn-Zr bone plate with CaP coating (a-g) and AZ31 bone plate with MAO coating (h-k). (a) Uncoated, CaP coated Mg-Nd-Zn-Zr and Ti bone plates; (b) operation on the tibia of a rabbit; (c) SEM images of CaP coating; (d) SEM images of cross-section of Ca-P coating; Radiographs of implants in tibias of New Zealand rabbits for 4 weeks after surgery: (e) uncoated Mg-Nd-Zn-Zr, (f) CaP coated Mg-Nd-Zn-Zr and (g) Ti. (h) A bone fracture defect model of 3 mm width magnesium plate implantation in the radius of New Zealand white rabbits. (i) SEM morphologies of MAO coated magnesium plates; (j) SEM morphologies of cross-section of MAO coating; (k) X-Ray Observation of the rabbits after 8 weeks postoperatively. Reprinted from Ref. [
While early works mainly focused on Mg alloying and surface modifications of Mg-based bone plates for internal fixation of fractures, the inferior mechanical properties, large amount of hydrogen to be released by Mg-based implants, especially to use large sized implants, and elevated local pH value still limit the clinical application of Mg-based metallic materials as bone plate materials, especially when they are used in the load-bearing site. Recent efforts are focusing on using Mg-based metals as a component of the whole internal fixation system to take advantage of Mg ions to be released during its degradation to accelerate the rapid fracture healing, which is the trend of the clinical transformation of Mg in bone fracture internal fixation field [22]. Zhang et al. developed an innovative hybrid system with Mg pins inserted into the stainless steel intramedullary nail to fix long bone fracture in rats. A larger callus was observed in the Mg group compared with the control group. The promotion role of Mg ions in bone fracture healing was confirmed again [141]. The underlying mechanism by which Mg ions promoted fracture healing was revealed by in vitro and in vivo tests [141]. First, Mg ions released by the degradation of Mg stimulated the dorsal root ganglion (DRG), leading to the rise of calcitonin gene-related peptide (CGRP) expression. Next, the rise of CREG expression enhanced osteogenic differentiation of the MSCs, which promoted the formation of a callus around the Mg implant. Finally, accelerated fracture healing was achieved [141]. Mg alone cannot provide sufficient mechanical support for stable fracture fixation at load bearing sites due to its rapid degradation in the early stage after implantation. Therefore, Mg is expected to be developed as an internal fixator for fracture fixation at non-load bearing skeletal sites, which limits the scope of its application in bone plates. Li Tian et al. [54] developed an innovative Mg/Ti hybrid fixation system for fracture fixation and healing enhancement at load-bearing skeletal sites. The Mg implant used for this hybrid system not only provided sufficient mechanical support but also promoted fracture healing through up-regulation of local CGRP secretion and acceleration of callus mineralization and its remodeling [22,54].
Many studies have shown that certain biomaterials with specific porous structures can enhance osteogenesis without incorporating osteoinductive biomolecules [142]. Pilliar et al. reported that enhanced bone remodeling was observed under the bone plate bonded with the porous surface. They ascribed this phenomenon to the more extensive stress transfer from bone to metal plate because of the good bone-to-implant bonding [143]. Fujibayashi et al. reported that porous Ti could become osteoinductive when it had a complex interconnecting porous structure and the surfaces could be bio-activated by simple chemical and thermal treatments [144]. Bohner and Miron demonstrated that intrinsic osteoinduction of porous biomaterials is originated from calcium and/or phosphate depletion due to poor ions exchange between the fluids in the porous biomaterials and their surrounding microenvironment [145].
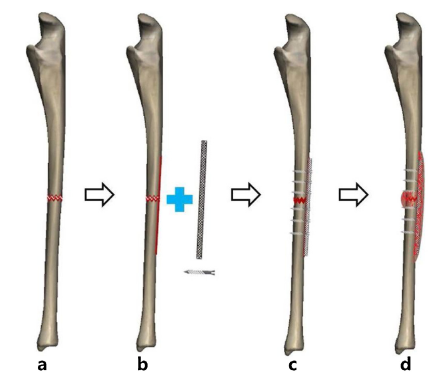
Hence, it is an important pathway for enhancing fracture healing and achieving bone-plate integration with porous plates. As shown in the Fig.16, we envisaged a kind of biological bone plate, which has a porous structure suitable for bone growth and a young's modulus similar to cortical bone. The lower elastic modulus avoids stress shielding and can ensure sufficient micro movement at the fracture region, thus activating the secondary bone healing and accelerating the fracture healing. At the same time, during the fracture healing, the porous bone plate can induce the bone tissue to grow into the bone plate and eventually cover the bone plate completely, so the bone plate does not need to be removed surgically or known as second operation for implant removal.
Fig. 16. Healing process of bone fracture fixed by porous bone plate. (a) The bone fracture; (b) A thin layer of cortical bone adjacent to the bone fracture site is removed; (c) The bone fracture is fixed by a porous bone plate; (d) Accelerate bone fracture is achieved and the bone plate and bone tissue grow together to form a whole.
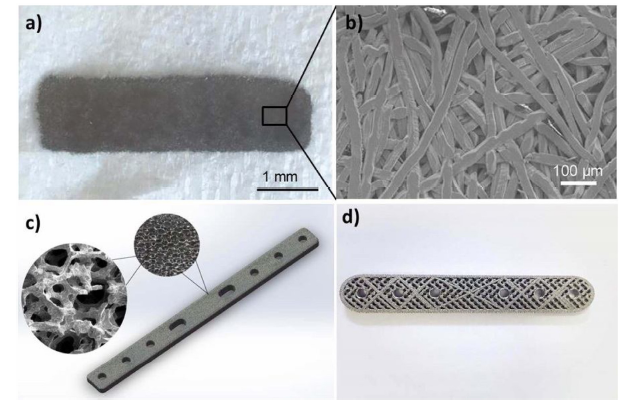
Takizawa et al. [146] prepared porous Ti fibre plates by moulding Ti fibres into plates by simultaneously applying compression and shear stress at normal room temperature (Fig.17a-b). They reported that Ti fibre plates had an elastic modulus similar to that of bone cortex, and stress shielding would not occur when the plate lied flush against the surface of bone. Ti fibre plates exhibited satisfactory effects when they were used to treat comminuted fractures. Additionally, it was expected that integration would be achieved between Ti fibre plates and their adjacent bone tissues through bone ingrowth to the plates, and there was no need for a secondary operation for implant removal. Therefore, it is a promising solution to design bone plates with a suitable porous structure to realize the concept of ideal bone plate.
Fig. 17. Porous bone plate. (a) A macroscopic image of a titanium fiber plate; (b) SEM image of a titanium fiber plate; (c) Trabecular porous Ta bone plate fabricated by chemical vapor deposition; (d) Porous Ta bone plate fabricated by combination of additive manufacturing and chemical vapor deposition. Reprinted from Ref. [
The effective modulus (Ep) of the porous metal to that (E) of the fully dense metal can be calculated by the Gibson-Ashby (GA) micromechanical model:
Ep=C×E×Rpn, (1)
where C and n are constants and Rp is the ratio of the density of porous metal to that of the fully dense metal [147]. Examples are Ti-6Al-4V alloy produced by electron beam melting (EBM) manufacturing (n = 2.10) [148], and a porous Ti was produced by the space holder method (space holder material; NH4HCO3; n = 2.00) [149]. Hence, the effective modulus of porous metal plates can be customized to match the modulus of the bone tissue by suitable porosity design. Torstrick et al. [150] studied the influences of porous structure on the osteogenesis and osseointegration of PEEK as load-bearing orthopaedic devices. The results showed that improved osteogenesis and osseointegration were achieved for the porous PEEK compared to smooth PEEK and Ti-coated PEEK.
Tantalum (Ta) is a well-known metal for medical devices because of its good biocompatibility. Ta has shown to be corrosion resistant and bioactive in vivo [151,152]. Therefore, Ta is gaining more attention as a new biomaterial. Porous Ta offers a low elastic modulus, high surface frictional characteristics and excellent osseointegration performance, which are all beneficial for eliminating stress shielding, increasing stress transfer from bone to plate and achieving bone-plate integration [153]. Based on these advantages, a porous Ta plate can be a candidate for the next generation of bone plate. We designed two kinds of plates made of porous Ta as shown in Fig. 17c-d; one was fabricated by coating Ta on an additive-manufactured (AM) porous Ti plate, and the other was fabricated by chemical vapor deposition (CVD). The plates were used to treat femoral fracture of sheep. Faster fracture healing and bone-plate integration was observed for the porous Ta plates [154].
The top priority of plate is providing essential mechanical fixation for the fracture ends, which is the basic premise for fracture healing. Neither currently known degradable biomaterials nor porous metallic biomaterials do well in mechanical performance. The plate must provide a balance of biomechanical performance and biofunction in order to achieve fracture healing success through reasonable structure design and materials selection. Revolutionary surgical techniques should be developed to cooperate with the clinical translation of the porous metal plate. It is recommended that a porous bone plate should mainly allow the bone to endure the loads after completion of bone formation by starting the use without loading and gradually increasing the load level to keep pace with the progression of bone union. At this stage, bone tissue has entered the spaces among the porous bone plate, providing unity between the porous bone plate and the neighboring bone [146].
Bone fractures are the most common traumatic injuries in humans. Currently, stainless steels and titanium-based bone plates remain dominant in bone fracture internal fixation. Although these alloys are rigid enough to ensure the fixation reliability for the fracture fragments, the undesired stress shielding effect and second operation for implant removal are unavoidable. In addition, these conventional bone plates have rather a poor performance in the treatment of the refractory fractures. In the past three decades, tissue engineering (TE) has been developed rapidly as a potential medical method to regenerate damaged tissues and organs. Its application in orthopaedics is one of the fastest growing fields, where TE is mainly used for the repair and regeneration of bone defects. Inspired by this, it is a promising direction to endow the bone plates with bioactivity (e.g. releasing biological factors) to enhance healing of bone fracture. Another strategy that may overcome the shortcomings of the traditional bone plates is from the angle of structure design, such as porous bone plates without sacrificing essential mechanical properties. Bone plates with porous structure can reduce stress shield and accelerate the bone fracture healing. Furthermore, the integration is expected to be formed between the bone tissue and the bone plates, and a permanent implantation could be achieved. Therefore, a second operation can be also avoided. As internal fixation implants for bone fracture, the top priority of the bone plates is to provide essential mechanical fixation for the fracture ends, which is the premise for fracture healing. Neither currently known degradable biomaterials nor porous metallic biomaterials do well in mechanical performance. The plate must provide a balance of biomechanical performance and biofunction in order to achieve fracture healing success through adequate structure design and material selection.
This work was supported by the National Key R&D Program of China (Grant No. 2016YFC1102000), the National Natural Science Foundation of China (Grant Nos. 81672139 and 81702129), the China Postdoctoral Science Foundation (No.171479), Doctor Initial Foundation of Liaoning Province (No. 20170520017), Affiliated Zhongshan Hospital of Dalian University (No. DLDXZSYY-DK201701), and by a grant from the Research Grants Council of the Hong Kong Special Administrative Region, China (Project No. T13-402/17-N).

 WeChat
WeChat
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}